Topic 01
Investigational targeted research
What the published research describes about investigational, research-stage approaches for solid tumors that overexpress voltage-gated sodium channels. Investigational and not FDA approved.
Plain-language education for people who want to understand advanced solid tumor cancer biology and the investigational research being studied. This is general information, not medical advice, and no treatment is offered here. For the full research record, see FixCancer.org.
Public Education Layer, Evidence at a Glance
Targeted Osmotic Lysis is investigational. Most published evidence is preclinical or veterinary, and the human evidence is limited to a single emergency-use case report. There are no published randomized trials, no human trials registered on ClinicalTrials.gov, and no FDA approval. Safety and effectiveness in humans are not established.
Verifiable references on PubMed, PMID 35453588, PMID 36230549, PMID 29643996, PMID 32486340, PMID 35967596, PMID 34201380, and PMID 39681070.
These are educational topics, not a menu of services. This site does not offer, recommend, or arrange treatment. Discuss any option with your licensed oncologist.
What the published research describes about investigational, research-stage approaches for solid tumors that overexpress voltage-gated sodium channels. Investigational and not FDA approved.
How second opinions and re-staging work through academic medical centers and NCI-designated comprehensive cancer centers. General education only, arranged through your own care team, not through this site.
Find trusted sourcesHow to understand clinical trials, early-phase research, and the FDA frameworks that govern investigational therapies. Trial searches are run through ClinicalTrials.gov and your care team.
How trials workHow to learn about advanced cancer and the research, and how to take questions to your own care team. Educational only, not medical advice.
Advanced cancer covers stage 3 and stage 4 disease. Stage 3 disease has spread to regional lymph nodes or nearby tissue. Stage 4 disease has metastasized to distant organs. The treatment plan changes when standard first-line and second-line therapies stop producing durable response.
Most patients reach this point after a sequence of surgery, chemotherapy, radiation, and immunotherapy. The next conversation should center on three questions. What therapies remain that have not been tried. What clinical trials match the tumor profile. What targeted approaches are available outside the standard pathway.
Targeted cancer therapy attacks specific molecular features of cancer cells. The features differ by tumor type. Some tumors over-express a surface receptor. Others over-express an ion channel. Targeted therapy uses that difference to selectively damage cancer cells while sparing normal tissue.
In the published research rationale, the aim is to concentrate activity on the tumor and reduce the side-effect burden associated with traditional cytotoxic chemotherapy. This describes the research goal. It is not a statement of proven benefit, and investigational approaches have not established safety or effectiveness in humans.
Hematologic cancers and bone marrow primary cancers fall outside the scope of solid tumor targeted therapy. Patients in those categories should consult a hematologist-oncologist directly.
People sometimes ask their oncologist about investigational research in situations like these. This is educational context, not eligibility criteria, and this site does not screen anyone.
Any such discussion belongs with a licensed oncologist, who reviews pathology, imaging, prior treatment, current performance status, and lab values. This educational site does not assess eligibility or schedule anything.
In the United States, the FDA oversees how investigational therapies are studied. Most access happens through enrollment in a registered clinical trial. In defined circumstances, expanded access and the federal Right to Try framework let a treating physician request an investigational therapy for a patient with a serious or life-threatening condition and no comparable approved option. This is general education. This site does not arrange access, screen patients, or maintain a treatment directory.
Start with the published research and the primary-source citations on FixCancer.org. Verify each cited PubMed identifier independently. Then discuss any option with your licensed oncologist. This educational site does not run an intake, assess eligibility, or arrange care, and it does not quote prices.
Plain-language basics drawn from the National Cancer Institute. This is general health information, not medical advice.
Cancer is a disease in which some of the body's cells grow uncontrollably and spread to other parts of the body. Normally, cells grow and divide to form new cells as the body needs them, and old or damaged cells die. Sometimes that orderly process breaks down. Abnormal cells grow when they should not, and they can form lumps of tissue called tumors.
Tumors can be cancerous or benign. Cancerous tumors invade nearby tissue and can travel to distant parts of the body to form new tumors. Many cancers form solid tumors. Cancers of the blood, such as leukemias, generally do not. There are more than 100 types of cancer, usually named for the organ or tissue where they form. Source: National Cancer Institute, What Is Cancer.
Cancer cells grow without the signals that normal cells wait for. They ignore signals that tell cells to stop dividing or to die. They can invade nearby areas, spread to other parts of the body, and hide from the immune system. Researchers study these differences to design therapies that target the abnormal features of cancer cells.
Stage describes how much cancer is in the body and how far it has spread. Knowing the stage helps a care team understand how serious a cancer is and plan treatment.
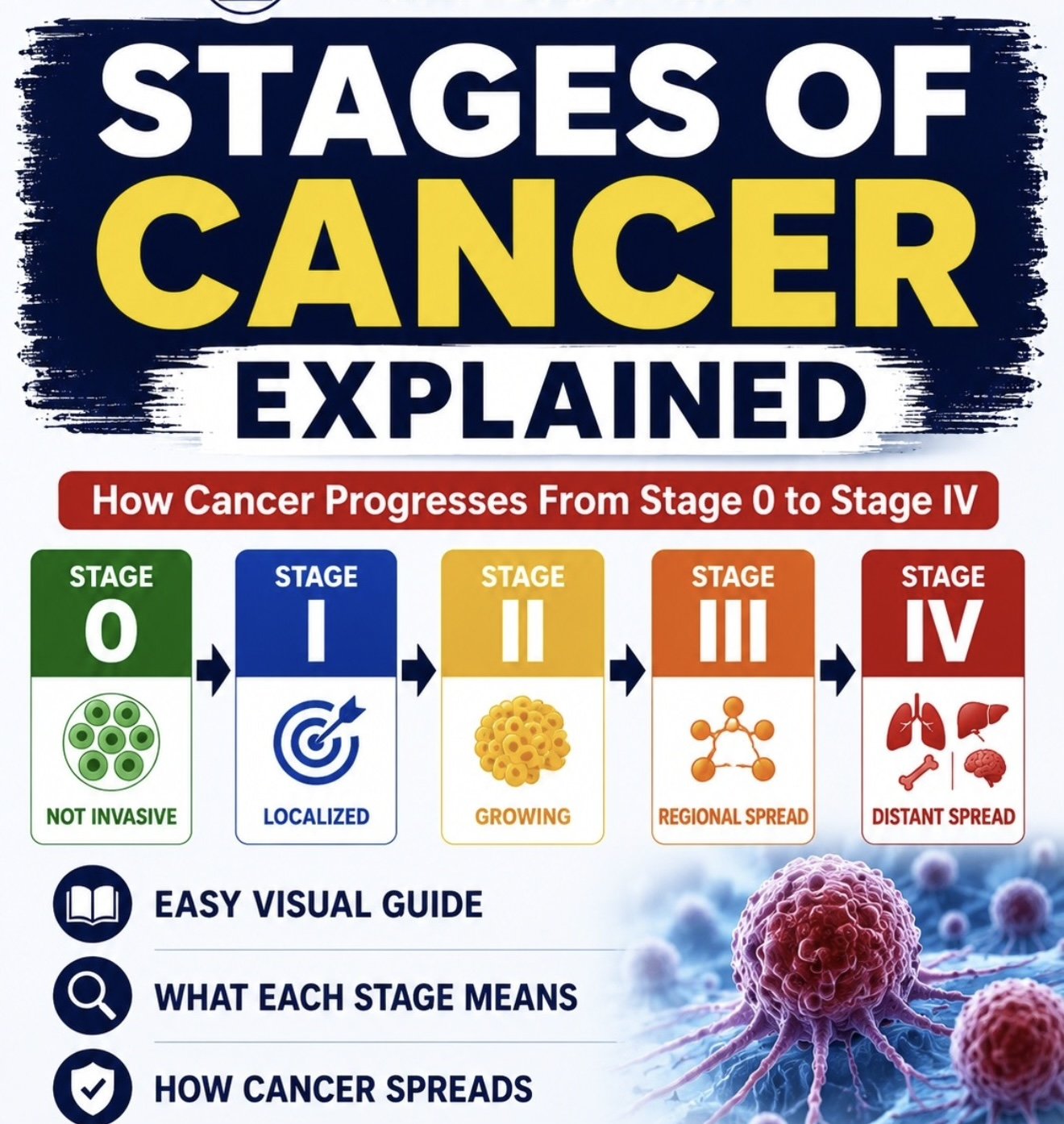
Most hospitals use the TNM system. T refers to the size and extent of the main tumor. N refers to the number of nearby lymph nodes that contain cancer. M refers to whether the cancer has metastasized, meaning it has spread from the primary tumor to other parts of the body.
A cancer registry may also describe cancer as in situ, localized, regional, or distant. A cancer is referred to by the stage it was given at diagnosis, even if it later changes. Source: National Cancer Institute, Cancer Staging.
Advanced cancer is a general term. It often refers to cancer that has spread and is unlikely to be cured, though treatment may still control it.
A cancer that has spread from where it first formed to another place in the body is called metastatic cancer. Metastatic cancer has the same name and the same type of cancer cells as the original cancer. Breast cancer that forms a tumor in the lung, for example, is metastatic breast cancer, not lung cancer.
For some people with metastatic cancer, treatment may help them live longer. For others, the goal of treatment is to control the cancer's growth or to relieve symptoms. Decisions about advanced cancer belong with a treating oncologist who knows the full medical picture, including pathology, imaging, and prior treatment. Source: National Cancer Institute, What Is Cancer and Metastatic Cancer.
Most people with cancer receive a combination of treatments. The types depend on the kind of cancer and how advanced it is. The list below summarizes the categories the National Cancer Institute describes.
Biomarker testing can help a patient and doctor choose among these options. Source: National Cancer Institute, Types of Cancer Treatment.
Clinical trials test new treatments in a series of steps called phases. Each trial has eligibility criteria that decide who can join.
Results from phase 1 through 3 trials inform decisions by agencies such as the FDA about approving treatments. You can search for cancer clinical trials through ClinicalTrials.gov and the National Cancer Institute, and your care team can help match a trial to a tumor's profile. Source: National Cancer Institute, How Do Clinical Trials Work.
An awareness summary of one area of published research. It is investigational, not an approved or proven treatment, and nothing here is medical advice.
Investigational means a therapy is still being studied and is not approved by the FDA. Investigational approaches have not established safety or effectiveness in humans through controlled trials.
One published line of research studies solid tumor cells that overexpress voltage-gated sodium channels. This approach, named Targeted Osmotic Lysis, appears in peer-reviewed laboratory studies, veterinary studies, and a single human emergency-use case report. There are no published randomized trials, no human trials registered on ClinicalTrials.gov, and no FDA approval. Safety and effectiveness in humans are not established. No claim of cure, benefit, or efficacy is made here.
The references can be verified on PubMed: PMID 35453588, 36230549, 29643996, 32486340, 35967596, 34201380, and 39681070. The full research record is documented at FixCancer.org. Discuss any option with a licensed oncologist.
Start with public, authoritative sources. These organizations publish accurate, current cancer information for patients and families.
Plain-language information on every cancer type, diagnosis, staging, and treatment. Contact Center 1-800-4-CANCER.
cancer.govA federal registry of clinical studies, including who is eligible and where trials take place.
clinicaltrials.govHealth information for patients from the National Library of Medicine.
medlineplus.govAcademic centers that offer second opinions, molecular profiling, and access to trials.
Find a centerNational Cancer Institute content is a work of the U.S. government and is cited and linked per NCI reuse guidance. No NCI text, images, or assets are reproduced on this page.
General educational answers. This site does not offer, recommend, or arrange treatment, and nothing here is medical advice.
Targeted cancer therapy is a research concept that focuses on specific molecular features of cancer cells rather than dividing cells in general. The research goal is to reduce damage to healthy tissue compared with traditional chemotherapy and radiation. This is a general description, not a claim of proven benefit.
Investigational means a therapy is still being studied and is not FDA approved. Investigational approaches have not established safety or effectiveness in humans through controlled trials. This site is educational and does not assess eligibility or arrange anything.
The published research studies solid tumor cells that overexpress voltage-gated sodium channels, in laboratory and veterinary models of breast, prostate, colorectal, lung, ovarian, pancreatic, gastric, and melanoma carcinomas. The literature describes hematologic and bone marrow cancers as outside that rationale. This is research context, not a statement that TOL treats any cancer in humans.
Second opinions are available through academic medical centers, NCI-designated comprehensive cancer centers, and patient navigation services. This educational site does not provide second opinions. Ask your care team how to request your pathology slides, imaging, and treatment summary.
No. This educational site does not offer treatment, quote prices, or arrange care. The cost of any medical care is set by licensed providers under applicable law, not by this site.
Most published evidence is preclinical or veterinary, with a single human emergency-use case report. There are no published randomized trials, no human trials registered on ClinicalTrials.gov, and no FDA approval. Safety and effectiveness in humans are not established.
FixCancers.com is an educational and awareness companion. FixCancer.org is the primary research home and documents Targeted Osmotic Lysis in detail. Both are educational and neither offers or arranges treatment.
FixCancers.com does not offer treatment, take appointments, assess eligibility, or quote prices. For decisions about your care, talk with a licensed oncologist. For trusted background reading, start with the National Cancer Institute. For the full research record on the science described here, see FixCancer.org.
Plain-language educational explainers, with sources. Educational information, not medical advice.
How to read the evidence and tell research from marketing. Educational information, not medical advice.